
Lung ultrasound has rapidly evolved from a niche imaging technique into a frontline diagnostic tool in emergency departments, intensive care units, and primary care settings. Today, clinicians are increasingly relying on lung ultrasound POCUS (Point-of-Care Ultrasound) to make fast, accurate, and bedside decisions without waiting for chest X-rays or CT scans.
This lung ultrasound guide is designed for emergency physicians, ICU teams, primary care physicians, medical students, and POCUS learners who want a practical, clinically oriented understanding of lung imaging. Rather than focusing on theoretical radiology, this guide emphasizes real-world bedside application; what you see, what it means, and how it changes patient management.
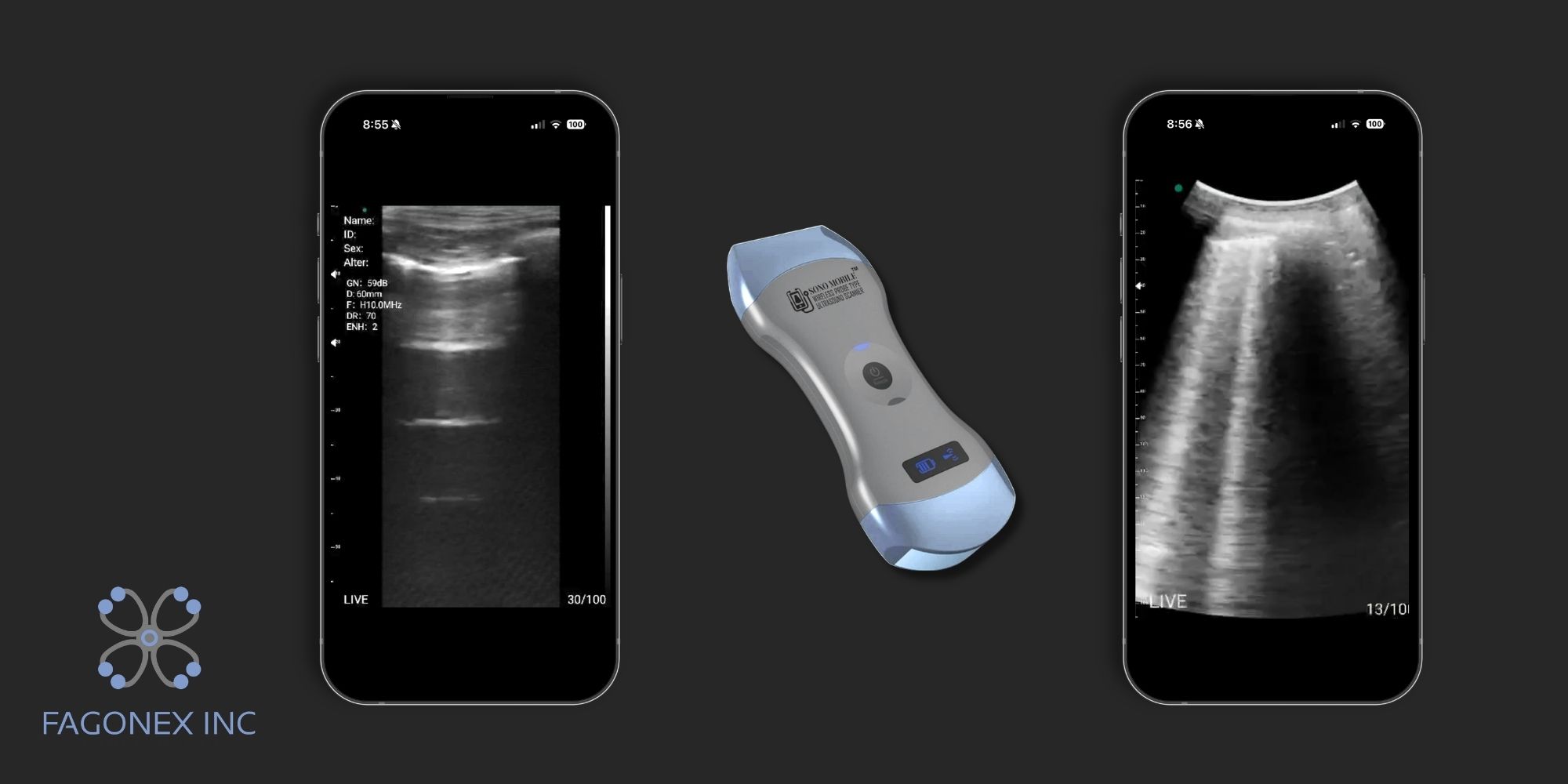
With modern handheld systems such as Sono Mobile™ CL64, lung assessment is no longer limited to radiology departments. It is now portable, immediate, and available wherever the patient is; resuscitation room, ward, ambulance, or rural clinic.
 Why Lung Ultrasound Is Important in Point-of-Care Care
Why Lung Ultrasound Is Important in Point-of-Care Care
Lung ultrasound is one of the most valuable applications of Point-of-Care Ultrasound because it is:
- Fast (results in seconds)
- Radiation-free
- Highly sensitive for many acute conditions
- Repeatable at the bedside
- Superior to chest X-ray in several critical scenarios
In emergency and ICU settings, time is often the difference between stabilization and deterioration. Lung ultrasound helps clinicians rapidly evaluate:
- Shortness of breath
- Hypoxia of unknown origin
- Chest trauma
- Suspected pneumonia or pulmonary edema
- Fluid overload states
- Pneumothorax suspicion
Unlike traditional imaging methods such as X-ray or CT scan, lung ultrasound provides dynamic, real-time information at the bedside, allowing clinicians to continuously observe lung behavior as the patient breathes and as their condition changes over time. Instead of capturing a single static image, lung ultrasound shows movement-based signs such as lung sliding, pleural motion, and evolving patterns of artifacts like B-lines or consolidations, which directly reflect physiological changes.
This real-time capability is especially valuable in critically ill or unstable patients who cannot be safely transported to the radiology department. In emergency rooms, intensive care units, and pre-hospital settings, moving a patient with respiratory distress, trauma, or hemodynamic instability can significantly increase risk. Lung ultrasound eliminates this need by bringing imaging directly to the patient’s bedside.
Clinicians can immediately assess conditions such as pneumothorax, pulmonary edema, pleural effusion, or pneumonia within seconds and then repeat the examination as often as needed to monitor progression or response to treatment. For example, after initiating diuretics in pulmonary edema, the reduction of B-lines can be tracked in real time, providing instant feedback on treatment effectiveness.
This makes lung ultrasound not only a diagnostic tool but also a continuous monitoring tool, improving decision-making speed, safety, and overall patient outcomes in acute care environments.

Basic Lung Ultrasound Anatomy and Artifacts
Understanding lung ultrasound begins with recognizing that most of what we see is not true anatomical imaging, but artifacts generated by air and fluid interactions.
The key structures include:
- Pleural line
- Rib shadows
- Lung sliding
- Vertical and horizontal artifacts
Because air blocks ultrasound waves, normal lung tissue is not directly visualized. Instead, clinicians interpret patterns created at the pleural interface.
These artifacts are not limitations; they are diagnostic signs.
Pleural Line, A-Lines and B-Lines
Pleural Line
The pleural line is a bright, horizontal echogenic line seen just below the ribs. It represents the interface between the visceral and parietal pleura.
A normal pleural line should appear:
- Thin
- Smooth
- Regular
- Moving with respiration
A-Lines
A-lines are horizontal reverberation artifacts that appear as repeating parallel lines beneath the pleural line.
They indicate:
- Normal air-filled lung
- Absence of interstitial syndrome
B-Lines
B-lines are vertical, laser-like artifacts that:
- Extend from pleura to bottom of screen
- Move with respiration
- Erase A-lines
They represent increased lung density due to:
- Pulmonary edema
- Interstitial pneumonia
- Fibrosis
- Acute respiratory distress processes
The number and distribution of B-lines are clinically important in assessing severity because they provide a direct, real-time indicator of the extent of interstitial involvement in the lungs. In lung ultrasound POCUS, a few isolated B-lines may be normal, but as their number increases and they become more diffuse or bilateral, they strongly suggest worsening pathology such as pulmonary edema, interstitial pneumonia, or acute respiratory distress processes.
Clinicians evaluate not only how many B-lines are present, but also how they are distributed across different lung zones. Focal B-lines may indicate localized disease, while diffuse, bilateral B-lines often reflect systemic or severe conditions. This makes B-line assessment a key component of any lung ultrasound guide, helping emergency physicians and ICU teams rapidly stratify disease severity and make timely treatment decisions at the bedside.
 Lung Sliding, Lung Pulse and Lung Point
Lung Sliding, Lung Pulse and Lung Point
Lung Sliding
Lung sliding is the shimmering movement of the pleural line during respiration. It confirms that visceral and parietal pleura are in contact. Its presence generally rules out pneumothorax at that location.
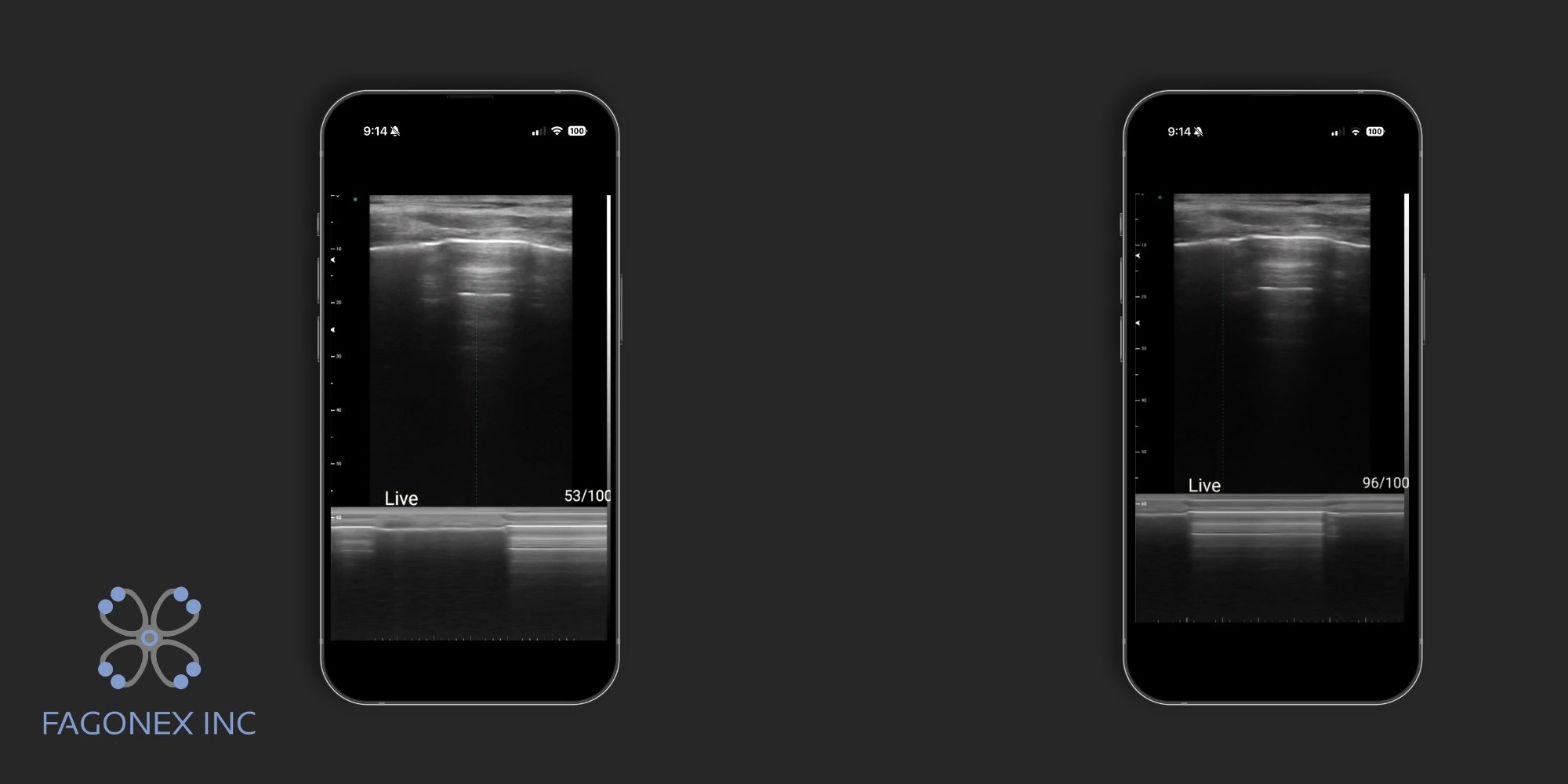
On M-mode ultrasound, this motion can be clearly assessed using devices such as Sono Mobile™ CL64. In normal lung sliding, the M-mode image shows the classic “seashore sign”, where the superficial tissues create parallel lines (the “waves”) and the moving lung below produces a granular pattern (the “sand”), reflecting normal pleural movement.
In contrast, when lung sliding is absent; such as in cases of pneumothorax, the M-mode displays the “barcode sign” (also called the stratosphere sign), where only horizontal lines are seen throughout the image, indicating a lack of pleural motion.
This M-mode comparison makes lung ultrasound particularly powerful in emergency medicine ultrasound, as it provides a rapid, objective way to confirm or exclude pneumothorax at the bedside, especially in emergency and critical care settings.
Lung Pulse
Lung pulse is a subtle, fine movement of the pleural line that is synchronized with the patient’s heartbeat rather than with respiration. Unlike lung sliding, which depends on breathing, lung pulse appears even when there is no ventilation. It is most useful in clinical situations where breathing is absent or minimal, such as during apnea, endotracheal intubation, or severe respiratory failure.
In lung ultrasound POCUS, the presence of lung pulse indicates that the pleural layers are still in contact, which helps differentiate complete lung collapse or apnea from pneumothorax. If lung pulse is present, pneumothorax is highly unlikely at that site. This makes it a valuable sign in emergency and ICU settings for rapid bedside decision-making and confirmation of pleural contact.
Lung Point
Lung point is the exact and highly specific transition zone on lung ultrasound where normal lung sliding disappears and the pattern of pneumothorax begins. In other words, it is the precise boundary between a normally aerated, sliding lung and an area where air has collected in the pleural space, separating the pleural layers.
When scanning the chest, the clinician may observe normal lung sliding in one area and absent sliding in another. The exact spot where these two findings meet is called the lung point. This finding is extremely important because it is considered almost 100% specific for pneumothorax, meaning that if you identify a lung point, pneumothorax is definitively present at that location.
The lung point can be dynamic, appearing and disappearing with respiration as the lung partially re-expands against the pneumothorax border. This makes it especially valuable in small or moderate pneumothorax cases, where other signs may be subtle or uncertain.
In lung ultrasound POCUS, identifying the lung point helps emergency and ICU clinicians confirm pneumothorax quickly at the bedside, allowing immediate clinical decisions without waiting for chest X-ray or CT imaging.
 Choosing the Right Probe and Scanning Preset
Choosing the Right Probe and Scanning Preset
Probe selection is essential for optimal imaging:
- Linear probe: Best for pleural line, pneumothorax, superficial detail
- Curvilinear probe: Best for deeper pathology like effusions and consolidation
- Phased array probe: Useful in cardiac-lung combined assessments
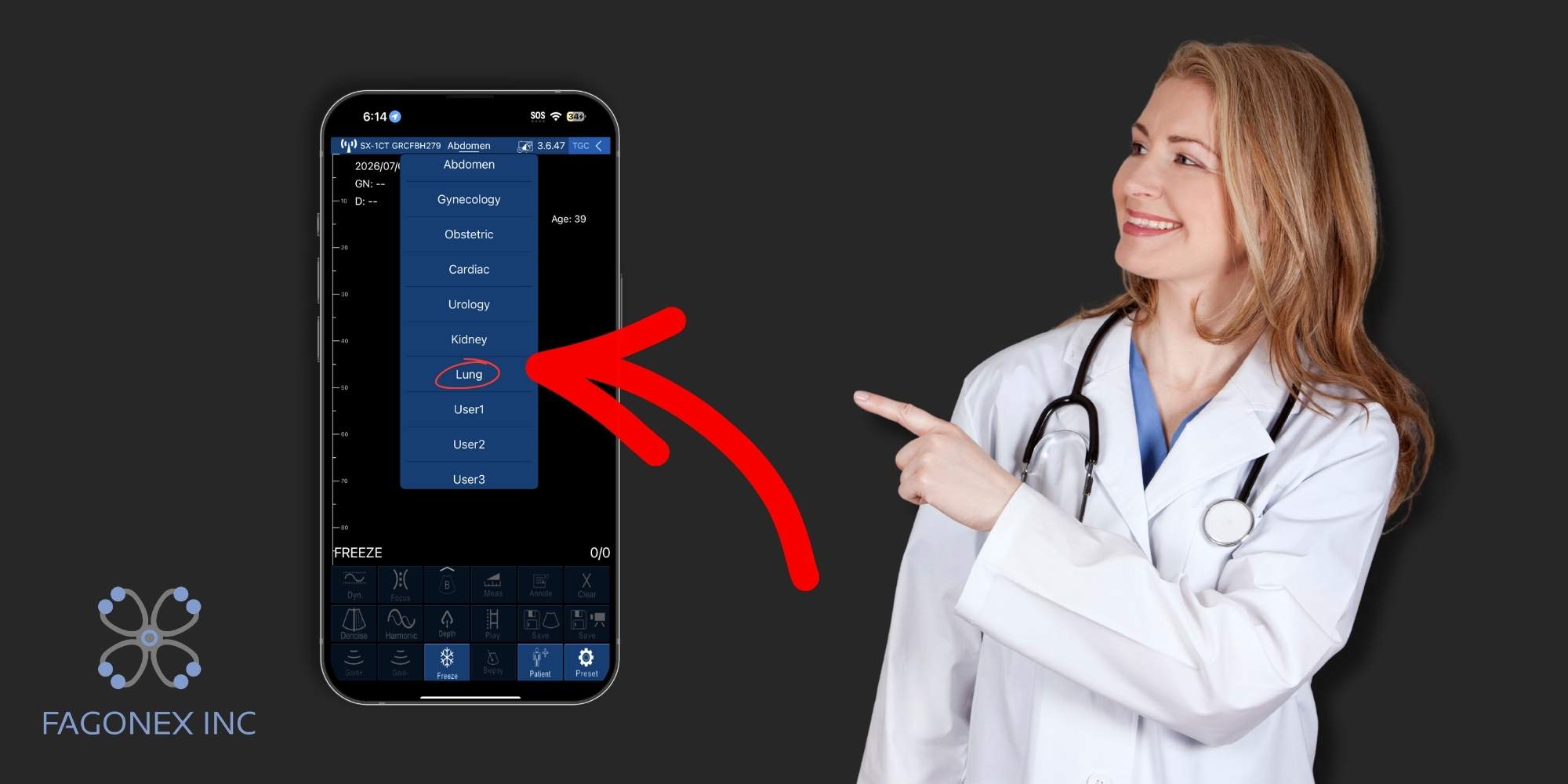
Handheld systems like Sono Mobile™ CL64 often allow automatic preset optimization for lung scanning, reducing setup time and improving workflow efficiency.
For clinicians comparing different device types, this handheld vs portable vs traditional ultrasound guide can help clarify the practical differences between bedside handheld systems, portable machines, and conventional cart-based ultrasound devices.

Step-by-Step Lung Ultrasound Scanning Technique
A structured approach ensures accuracy:
- Position the patient (sitting or supine depending on condition)
- Start at the anterior chest (2nd–4th intercostal space)
- Scan longitudinally between ribs
- Move systematically to lateral and posterior zones
- Compare both lungs side by side
- Document findings in each zone
A common approach divides the chest into 6–12 zones for systematic evaluation.
Consistency is more important than speed in early learning stages. For students, residents, and POCUS learners, structured practice with handheld ultrasound in medical education can help build confidence in probe handling, artifact recognition, and bedside interpretation.
Normal Lung Ultrasound Findings
Normal lung ultrasound includes:
- Clear pleural line
- Lung sliding present
- A-lines dominant
- No B-lines or minimal isolated B-lines
This pattern suggests normal aeration and excludes major pathology in most acute settings.
Pneumothorax on Lung Ultrasound
Pneumothorax is one of the most important life-threatening conditions detectable by lung ultrasound.
Key signs include:
- Absence of lung sliding
- Absence of B-lines
- Presence of A-lines only
- Possible lung point (confirmatory)
Lung ultrasound is more sensitive than chest X-ray in detecting early pneumothorax, especially in trauma or ventilated patients.
 Pleural Effusion on Lung Ultrasound
Pleural Effusion on Lung Ultrasound
Pleural effusion appears as an anechoic or hypoechoic fluid collection above the diaphragm.
Findings include:
- Fluid layer above diaphragm
- Floating lung tissue (“jellyfish sign” in large effusions)
- Compressive atelectasis in adjacent lung
Ultrasound can detect even small effusions that are often missed on X-ray.
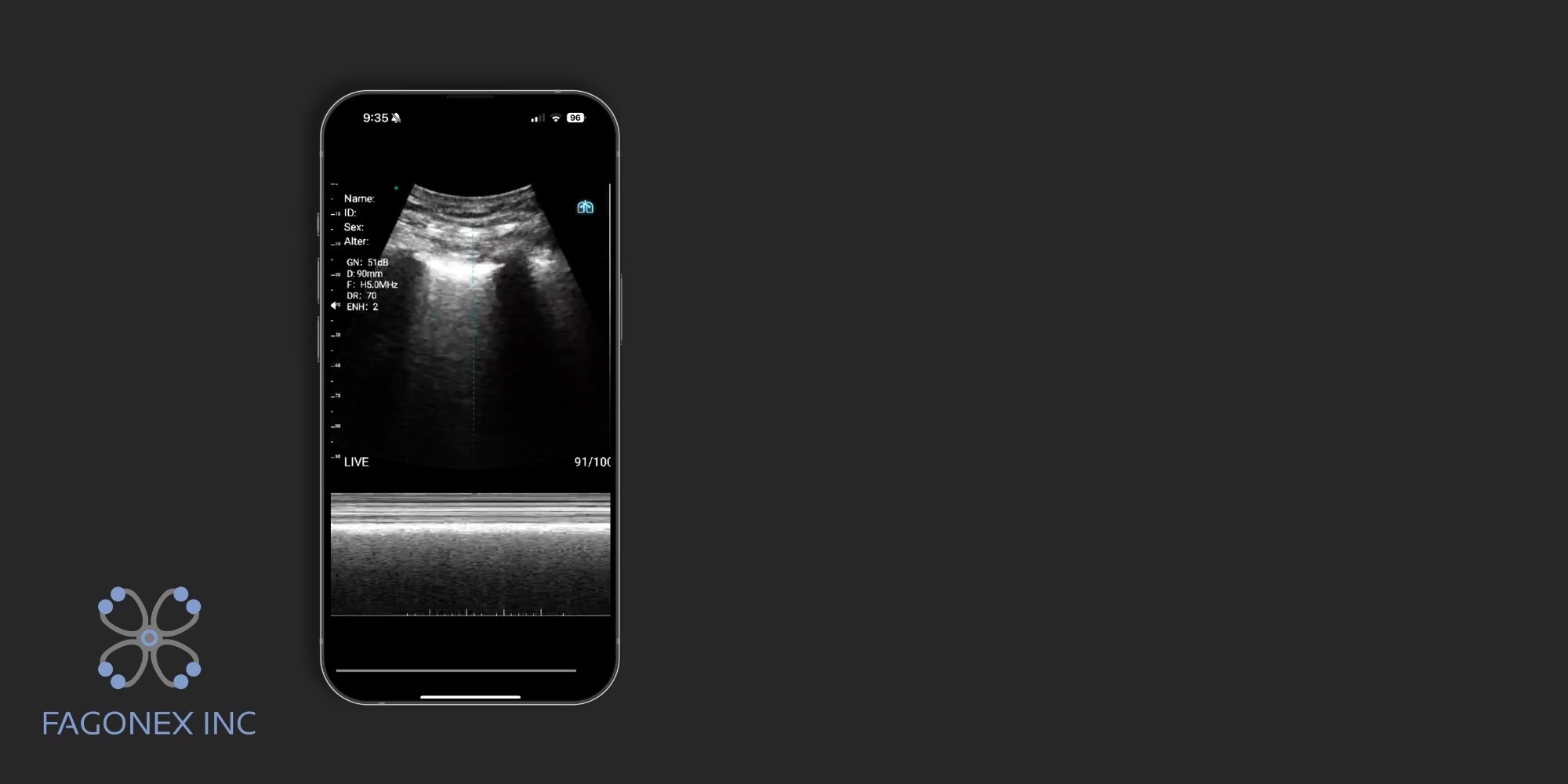
Pulmonary Edema and B-Lines
Pulmonary edema produces multiple bilateral B-lines due to interstitial fluid accumulation.
Typical pattern:
- Diffuse, bilateral B-lines
- Symmetric distribution
- Preserved pleural sliding (early stages)
This is especially useful in differentiating cardiac failure from other causes of dyspnea.
Lung Consolidation and Pneumonia Patterns
Lung consolidation appears as tissue-like (“hepatization”) lung.
Key findings:
- Hypoechoic or tissue-like area
- Air bronchograms (static or dynamic)
- Irregular pleural line
- Possible pleural effusion
Ultrasound is particularly sensitive for peripheral pneumonia and is increasingly used in emergency diagnosis.
 Lung Ultrasound Protocols: BLUE, eFAST and Bedside Screening
Lung Ultrasound Protocols: BLUE, eFAST and Bedside Screening
Several standardized protocols help clinicians structure their evaluation:
BLUE Protocol
Used in acute respiratory failure to differentiate causes like:
- Pneumonia
- Pulmonary edema
- COPD/asthma
- Pneumothorax
eFAST
Extended FAST exam used in trauma:
- Detects pneumothorax
- Identifies hemothorax
- Evaluates abdominal bleeding
Bedside Screening
Simplified zone-based scanning used in ICU and primary care for rapid assessment and follow-up.
For broader bedside workflows, portable ultrasound solutions allow clinicians to select handheld systems and accessories that support different clinical environments and scanning needs.
Common Mistakes and Interpretation Pitfalls
Even experienced users may make errors:
- Confusing subcutaneous emphysema with B-lines
- Misinterpreting rib shadows as pathology
- Overcalling B-lines in dependent lung zones
- Missing small pneumothorax due to incomplete scanning
- Not comparing both lungs systematically
Training and repetition are essential to avoid misinterpretation.
Documentation, Image Storage and Follow-Up
Proper documentation improves clinical value:
- Record labeled lung zones
- Save representative clips (sliding, B-lines, effusion)
- Compare serial scans over time
- Integrate findings into clinical notes
Modern POCUS systems and handheld devices enable direct image storage and integration into hospital systems. In mobile and wireless workflows, wireless ultrasound probes can also support flexible image acquisition, portability, and bedside use across different clinical settings.
How Handheld Ultrasound Supports Faster Lung Assessment
Handheld ultrasound has transformed bedside lung evaluation. Devices like Sono Mobile™ allow clinicians to perform lung assessments anywhere:
- Emergency departments
- ICU bedsides
- Ambulances
- Rural clinics
- Home visits
Key advantages include:
- Immediate diagnosis without delay
- Reduced dependence on radiology
- Improved triage decisions
- Faster treatment initiation
- Cost efficiency in acute care workflows
For time-critical conditions like pneumothorax, pulmonary edema, and pneumonia, handheld lung ultrasound significantly improves clinical response time.
In outpatient and community environments, primary care ultrasound can also help clinicians expand access to fast bedside assessment without depending entirely on referral-based imaging.
Conclusion
Lung ultrasound has become an essential skill in modern bedside medicine. With its ability to rapidly detect pneumothorax, pleural effusion, pulmonary edema, and pneumonia, it is now a cornerstone of POCUS practice.
This lung ultrasound guide provides clinicians and learners with a practical framework to interpret pleural anatomy, recognize artifacts, and apply structured protocols such as BLUE and eFAST.
As healthcare continues to shift toward faster, decentralized diagnostics, handheld systems like Sono Mobile™ are playing a key role in expanding access to high-quality imaging. For emergency physicians, ICU teams, and primary care clinicians, lung ultrasound is no longer optional; it is becoming essential for modern patient care



